The health care service system in Japan is delivered by mandatory, non-profit public health insurance systems, and not by the service providers for profit. Japan’s public health insurance system is composed of three types of health insurances: occupation-based, municipality-based, and a separate system for persons 75 years old and over. Every resident in Japan must belong to a public insurance as an enrollee. All health insurers are not-for-profit organizations. Health services are provided not only by public providers, but also private ones which satisfies the “non-profit” principle. Patients enjoy “freedom of choice,” which assures people can select and contact the physicians in any medical institutions. The cost of medical care is financed through insurance premiums, tax revenues, and copayments. Elderly, infants and low income people are completely or partially exempted from copayments. Other people must pay copayments which are 30% of the total medical cost when they use medical services. According to income level and age of patients, the maximum amount of copayment is determined. Sustainability of the system depends on whether the inter-institutional redistribution of the burden can work or not, and whether enough human resources are available for service provision to elderly.
Social Security in Japan 2014
Chapter 4 Health Care
4.1 Introduction
4.2 Public Health Insurance
Health insurance system in Japan has been continuously developing since the 1920s. At first, the Health Insurance Act was enacted in 1922. While occurrence of the Great Kanto Earthquake in 1923 made the enforcement of the law delayed until 1927, this public health insurance covered “blue color” workers in the factory and the mine. Secondly, the National Health Insurance act was enacted in 1938. This law widened the coverage of public health insurance not only to farmers, but also to the general public not covered by the Health Insurance Law. The National Health Insurance Law prescribed that municipalities could be insurers of the national health insurance for the people living in their regions. However, the law permitted that municipalities could choose not to establish the national health insurance, and that people could enroll the public health insurance by their decision. Hence there remained non-insured people. From 1939 through 1941, other public health insurance law started to cover the “white color” workers, including government officials. Furthermore, the public health insurance system also started to cover seaman by Seamen’s Insurance Act in 1940. In summary, before WWII, the public health insurance system in Japan gradually developed by enacting different health insurance laws for each sub-group in the whole society.
Public health insurance developed further after WWII. Laws on public health insurance which had been enacted before the end of the WWII were consecutively used after the war. Hence the public health insurances had been taking over the characteristics before. Each law of public health insurance regulated its own financial budget, therefore their managements had been independent from each other. More importantly, lack of the law for comprehensive health insurance coverage implied that there remained the possibility that non-insured people existed. This defect was improved by the enforcement of the new National Health Insurance Act in 1961, with which Japan attained universal coverage. The new National Health Insurance Act mandated all residents in Japan to enroll in the national health insurance, except in the case that they have already enrolled in other public health insurances.
The next issue of development of the public health insurance was the improvement of the insurance benefit, and improvement of the inequality in insurance benefit among different schemes. In the early 1960’, expensive antibiotic drugs some steroid drugs and drugs for chemotherapy had been prohibited to use in public health insurance system. This restriction was abolished in 1962. It raised the health care cost, but the expanded cost was absorbed into the expanded financial surplus in the public health insurance system, owing to the high rate of economic growth.
In the early 1960’, copayment rate was 50% for all of enrollees in the national health insurance, while it was 0% for the head of the household (principal enrollee) of the Society-managed Health Insurance and Association-managed Health Insurance. Thus the amount of the subsidy from the government to the insurers in the national health insurance was increased, in order to lower the copayment rate for the enrollees in the national health insurance.
The burden of copayment tended to be lager for patients with severe diseases or with chronic diseases. In 1960s, the municipalities started to subsidize the elderlies (over 70 years and older) so that their copayment rate became 0%. This subsidy to copayment for the elderly became universal in 1973. For people less than 70 years old, the High-cost Medical Care Benefit System was introduced also in 1973 to cap the burden of copayment.
In early 1970s, the oil crisis hit the Japanese economy. To prevent the rapid price increase, the government implemented policies to control economic activities, such as cutting public spending. These policies were successful, and then the recession came next year. It reduced the financial revenue of the government as well as the premium revenue of the insurers of the public health insurance system. The government started to fill the annual financial gap by issuing the national bond, and the governmental spending started to be reduced. Social security spending also started to be contained, along with the governmental subsidy to it.
In spite of the reduction in social security spending, the health care expenditure for elderly had been rapidly increasing. One of the reasons was the governmental subsidy to the copayment for the elderly. The health care cost for the elderly increased from 40 billion yen in 1973 to 67 billion yen in 1974, and to 87 billion yen in 1975. After 1975, the growing rate was very high. To contain the rapid cost increase, the new health care system for the elderly was needed. But the cost increase was not the only reason for the introduction of the new system. At that time, the elderly had only medical care services, not the services for the health promotion, preventive measures such as health check-ups, rehabilitation or nursing care. These services in collaboration with the medical care were needed to be supplied in a more integrated manner. Hence in 1983, the Health Service System for the Elderly was introduced. Per-diem basis copayment was introduced for medical care utilization.
The Health Service System for the Elderly is a part of inter-institutional fiscal adjustments with respect to health care cost for elderly. Since the mid-1980s, cost containment policies had been employed. Inequality of copayment rates between the different public health insurances were equalized to 30% in 2003. Inter-institutional fiscal adjustments with respect to health care cost for elderly had been strengthened, and it developed to the Medical Care System for Elderly in the Latter Stage of Life in 2008.
As stated before, Japan’s medical services are financed through a public mandatory health insurance system, which is composed of three types of public health insurances: occupation-based, municipality-based, and separate health insurance for persons 75 years old and over. The elderly aged 75 or over enroll in public health insurance, which is called Medical Care System for Elderly in the Latter Stage of Life. Those who are below 75 years old enroll in occupation-based public health insurance or National Health Insurance. There are three types of occupation-based public health insurance. One is the health insurance for workers at firms of a certain size which are called the Society-managed Health Insurance. Each Large company has a duty to establish each firm based non-profit public health insurers to provide public health insurance coverage to their employees. For those who work at smaller firms, the Japan Health Insurance Association, which is the public association for the health insurance, provides a collective health insurance, which is called the Association-managed Health Insurance. In addition, special professions such as civil servants, private school teachers and employees, day laborers and seamen, form separate nation-wide professional associations.
Those who are below 75 years old and not covered by occupation-based public health insurance are covered by a National Health Insurance. The insurers of National Health Insurance are the municipalities, the local government which are closet to the community. This scheme covers self-employed people, workers engaged in agriculture, forestry and fisheries, workers of small businesses, the unemployed and pensioners.
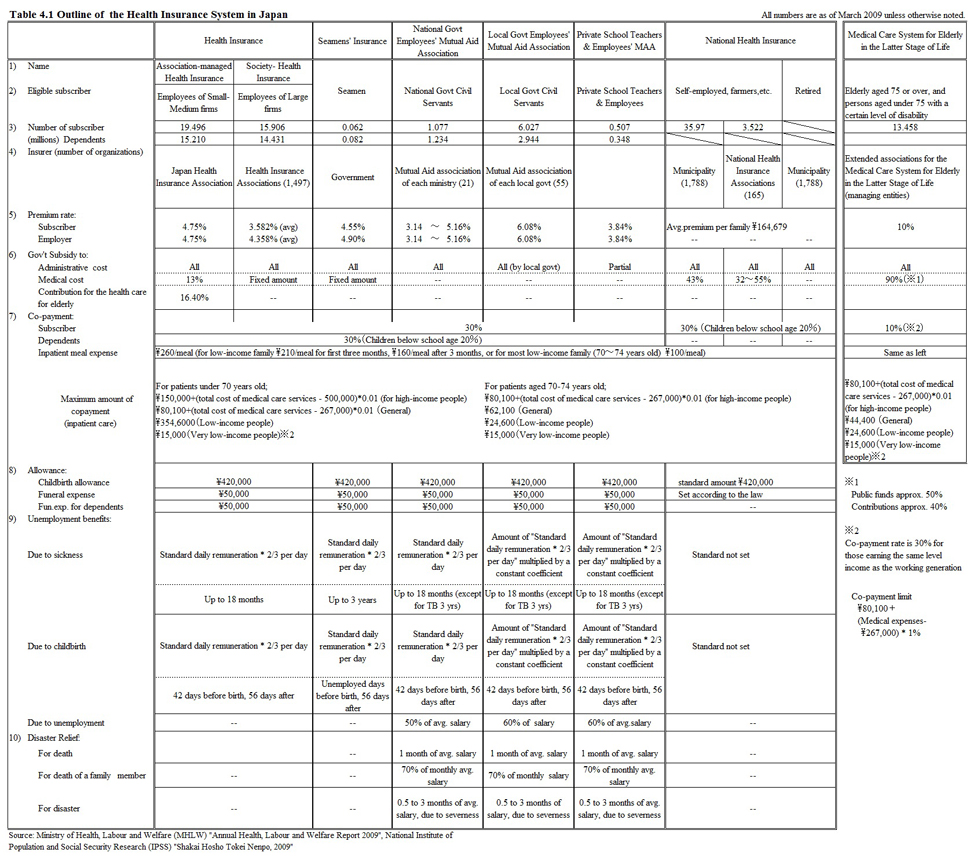
These public health insurances provide universal coverage of the population in Japan. The outline of each system is shown in Table 4.1 (located at the end of this chapter). The National Health Insurance covers 31% of the total population, 27% for the Association-managed Health Insurance, 24% for the Society-managed Health Insurance, and 11% for the Medical Care System for Elderly in the Latter Stage of Life.
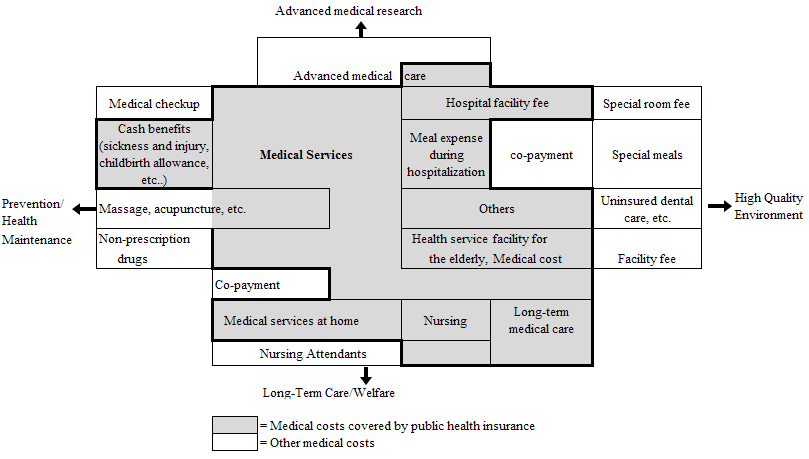
Insurance benefits are standardized throughout all public health insurance schemes. As shown in the Figure 4.1. The extent of the medical services covered by the public health insurance is discussed in the Central Social Insurance Medical Council, which members are consisted of representatives of clinical physicians and hospitals, of insurers in public health insurances, and of the general public. The council also discusses about the official tariffs of medical services. Based on the suggestions from the council, the Ministry of Health, Labor and Welfare decides the coverage and prices of the medical services.
Generally speaking, the individual’s health care expenditure is higher as her/his age is higher. This is also true in Japan. Hence the average health care expenditure per enrollee is highest in the Medical Care System for Elderly in the Latter Stage of Life (\844,382 /year), because individuals more than 75 years old enroll in it, as we have already explained. Most of individuals aged between 65 and 74 enroll in the national health insurance, so that average health care expenditure per enrollee is \168,658 /year, higher than the ones in other occupation- based health insurances. The costs of the health benefit in public health insurances reflect this difference of enrollees’ age structure as shown in the upper part of the Table 4.2.
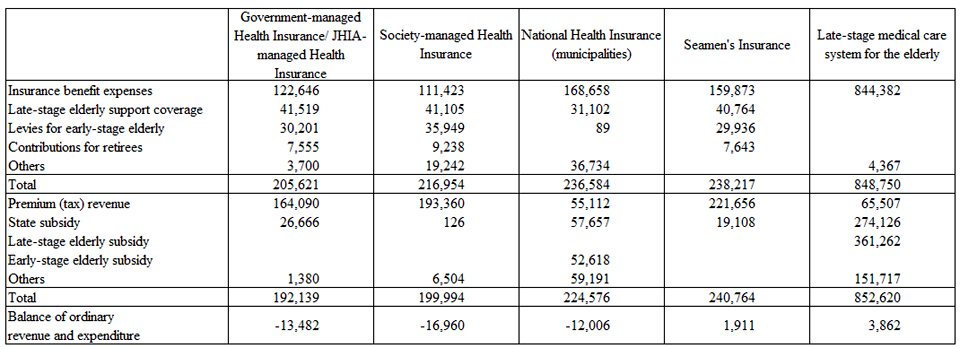
Source: Ministry of Health, Labor and Welfare (MHLW), “Annual Health, Labor and Welfare Report 2012”
The public health insurance schemes are financed by premiums, subsidies from the general budget of the government, and co-payment from patients. Insurance premiums are one of the main financial resources for the public health insurance. Their methods of premium collection are different among the public health insurance schemes. Insurers of occupation-based public health insurance collect the premium by deducting the salaries. The lower and upper limits of the premium are set at 30/1000 and 120/1000, respectively. The premium of the National Health Insurance is collected through the direct payment to the municipality government by the subscribers on household basis. The premium consists of a proportional part based on the income, assets, and number of people in the household and a fixed part per household. Insurers in Medical Care System for Elderly in the Latter Stage of Life collect the premiums mainly by deducting the pension paid to the elderly.
Central, prefectural, and municipal governments subsidize the insurers of the National Health Insurance for their running cost. Central government subsidizes the 41% of the health care benefits, and the prefectural governments subsidize 9% of that. This amounts to \57,657 per enrollee as shown in Table 4.2. In case the insurance finance faces a deficit, the managing municipality will bear the cost as a form of subsidy to the insurer. This amount is included in the category “others” in revenue in Table 4.2. We can see in Table 4.2 that insurance benefit cost is higher in the National Health Insurance and the Medical Care System for Elderly in the Latter Stage of Life, but premium revenue is lower in these two insurances. This causes a fiscal imbalance in these two insurances. To adjust the fiscal imbalance, inter-institutional fiscal adjustments have been introduced. Under this scheme, burdens of the health care cost for the elderly aged between 65 and 74 are reallocated among the insurers of public health insurance. The amount which the National Health Insurance receives from this fiscal adjustment is \52,618 per enrollee.
The Medical Care System for Elderly in the Latter Stage of Life for those aged 75 and older itself can be regard as a scheme for inter-institutional fiscal adjustments. The elderly aged 75 and over enroll in this system, and they must pay premiums. This premium finances 10% of the medical costs. Of the remaining 90%, 50% is covered by central and local governments’ subsidies and 40% by contributions from insurers of other insurance programs. The amount which the medical care system for elderly in the latter stage of life receives from this fiscal adjustment is \361,262 per enrollee.
Table 4.2 does not show the co-payment but the total amount of copayment is not negligible, as the co-payment rate is basically 30% for public health insurance systems in Japan. Payment is made every time a visit is made to a medical institution. Co-payment rate varies according to patients’ age and income, such as 20% for children below school age, or 30% for the high-income elderly more than 70 years old, who earn the same level of income as the working generation, 10% for most of the elderly more than 75 years old. The statutory co-payment rate is 20% for the elderly aged between 70 and 74, whose income levels are not so high. However, the co-payment rate for these people is temporally at 10% mobilizing a budgetary measure.
The High-cost Medical Care Benefit is applied to all public health insurance. This system aims to hold down the co-payment amount by setting a cap according to age and income, and the insurer bears the difference between the cap and the payable co-payment amount. The cap amount is set lower for low-income earners. For example, the monthly cap for a low-income earner aged under 70 is \35,400, and under the Medical Care System for Elderly in the Latter Stage of Life, low-income earners only pay up to \8,000 for outpatient treatment, and up to \24,600 for hospitalization.
As the aging of the population is still proceeding, the health care costs for the elderly will increase accordingly. This automatically increases the occupation-based insurances’ burden of subsidy to the Medical Care System for Elderly in the Latter Stage of Life. The increased burden should be covered by increased amount of insurance premium in those insurances. However, the insurers’ financial situations vary and it may be too heavy burden for some insurers. To make the burdens more equitable, the policy has changed to determine the amounts of subsidy by the total amount of enrollees’ income. By this policy, insurers of occupation-based health insurances raise the premium rate only when their premium level is too low for the income level of their enrollees.
The National Health Insurance has a larger number of lower income subscribers and elder subscribers than the occupation-based health insurances. As a result, the relatively poorer enrollees are confronting the relatively higher premium rate. This leads to an increase of the unpaid insurance premium in the national health insurance. In 2011, the amount of unpaid insurance premium was 10.6% of the total amount of levied premiums. In social insurance system, the unpaid insurance premium means they lose the eligibility, and moral hazard occurs. To avoid this, target groups of the premium payment exemption have been enlarged. Also, extremely poor households are guaranteed access to medical services without the payment of premiums, based on the Public Assistance system.
4.3 Service provision
The fundamentals of the medical care provision systems were constructed before WWII. Management of the medical institutions satisfies the “non-profit” principle while owners of the medical institutions include the public and the private. Medical doctors are educated with a six years university education program and trained with five years training program after graduation. They can educate themselves to deepen their clinical specialties. General practice has not been explicitly recognized as one of clinical specialties, so that there are no general practitioners as clinical specialists. There has been no gate-keeping system. Patients can choose the medical institutions they want to visit. Therefore, the roles of community clinic and specialized hospitals have not been clearly separated. A patient can choose for their first contact the specialist in hospital outpatient department. In the mid-1970s, the copayment rate for elderlies was set at 0%. Evidently, it had inflated the usage of medical care among the elderlies. However, this was a precarious measure taken due to the scarcity of long term care facilities in those days. The 0% copayment rate was abolished in 1983 and together with the policies of increasing the long term care facilities, the efficiency in provision of the inpatient care services for elderly has been improved by the policies amendment of the medical institution law, and the policy inducement by the changing tariff for medical care services. Introduction of the Long Term Care Insurance created many alternatives for elderly who need life support services other than inpatient care in hospitals. Now the issue is how to coordinate the medical care and the long term care.
Before the Meiji era, physicians existed in Japan who were called “Kusushi” based on the oriental medicine at that time. They made diagnose, decided the prescription, and sold the pharmaceuticals to the patients. However, they were excluded from the practice by the certification regulation which replaced them by the physician educated by Western medicine introduced in the Meiji era.
Medical doctors sold pharmaceuticals to patients while they were educated on Western medicine. This was because there were few pharmacists at that time. Pharmacists hoped to achieve the separation of medical practice and drug dispensing, but it could not be attained, because of their weaker political power. Hospitals based on Western medicine were first established at Nagasaki in 1861. The number of hospitals increased to 106 in 1878. Hospitals were established by the central government, local governments, and private citizens and organizations. In those days, there was no public health insurance. Hence poor people could not access medical care services. Japan Red Cross was established as the Hakuai-sha in 1878, and Social Welfare Organization Saiseikai Imperial Gift Foundation (The Saiseikai) was established in 1911. They constructed hospitals and started to provide the medical services to the poor.
In those days, physicians could start their private practice where they preferred (free-entry). Hence medical institutions were located densely at the urban areas because the medical doctor as the manager of medical institution wanted to keep their financial status better. This made accessibilities to the medical care unequal among geographic areas. In rural areas, for example, physicians could not earn enough bread because farmers were relatively poorer than other people, and could not pay the fee of the medical care services. On the other hand, it was said that physicians were so competitive in urban areas that they also could not earn their enough bread in those areas. After WWII, the hospitals and clinics lost their functioning, personnel working in them, and even their buildings due to the results of the war. To increase the supply of medical care services, various policies were employed. Medical institutions controlled by the Department of the Navy and by the Department of War were merged into the Ministry of Health and Welfare, and those medical institutions were made available for utilization of the general public as the National Hospitals. The central government of Japan decided to make financial subsidy to private (but not for profit) medical institutions for their investment to hospital/clinic construction and/or medical equipment. Because of these policies and the effects of the long-lasting economic booms, the number of private hospitals and clinics expanded.
Local governments, as before WWII, established their hospitals and clinics. The Japan Red Cross, the Saiseikai, and other non-profit organizations also established medical institutions. These new investments contributed partly to the gradual improvement of the distribution of medical institutions. However, there has been no effective method to cure the geographical inequality of medical institutions distribution. In the mid-1980s, it was pointed out that regional variations of the inpatient care cost correlated to the supply of the inpatient beds. The medical institutions law was amended so that the government could specify the area where the inpatient beds were over-supplied relative to the number of population in 1985.
Among the amendments of the medical institutions law since then, the second amendment of the law introduced the hospital categorization of Special Functioning Hospitals and the bed type categorization of “Long-term Care-type Beds” in 1992. Special Functioning Hospitals is a classification of the hospitals which provided high-technology and intensive inpatient care. The bed type categorization of “Long-term Care-type Beds” was introduced because the utilization of the beds was not necessarily based on the medical needs. In those days, as we have seen in section 4.2.1, the copayment rate for the elderly was 0%. This policy made the patients who needed support for living rather than medical care, utilize the unnecessarily inpatient care.
The Long Term Care Insurance law was enforced in the year 2000. Since that time, utilization of most long-term care beds was reimbursed not by the public health insurance, but by the Long Term Care Insurance. By the introduction of Long Term Care Insurance, the patients who had relatively less need for inpatient medical care were induced to use life support services.
The acute inpatient care was also reformed so that the services could be more efficiently supplied. In 2003, Diagnosis Procedure Combination (DPC) was introduced for trial as the classification tool of diseases. The reimbursement system for the acute inpatient care started to use the DPC in 2006. Reimbursement based on DPC is per diem basis. Hence it has no direct effect to shorten the average length of stay.
One of the characteristics of the Japanese health care system is the availability of beds and the long duration of stay in medical facilities. By definition, in the medical institution law, clinics can have less than 20 beds, while hospitals must have 20 beds or more. In 2012, there were 8,565 hospitals, 100,152 clinics, and 68,474 dental clinics in Japan. The number of beds in hospitals is 1,578,254 (12.4 beds /1,000 people), and the number of beds in clinics is 125,599 (0.99beds / 1,000 people). The average length of stay in the hospital is 31.2 days for hospitals and 17.5 days for clinics, which is much longer than 8 days for OECD countries.
Secondly, there exists no explicitly defined general practitioner, so that we have essentially no gate-keeping system. Medical doctors are educated for medicine in six year undergraduate courses. They must pass the National Medical Practitioners Qualifying Examination. After passing the examination, they are trained as a medical doctor in a five year post-university education course. After finishing the post-university education course, they are educated as specialists in their clinical specialty. The total number of medical doctors working in medical institutions is 288,850 (2.4 persons /1,000 people), 188,306 working in hospitals, and 100,544 in clinics. There are few foreigners who are working as clinical medical doctors; 1,580 in hospitals and 828 in clinics.
Thirdly, there is no nationally qualified nurse practitioner, who can practice nursing care independently, while the number of registered nurses who are working in hospitals is 725,560. They can work as registered nurses after a minimal three years education, and passing the national nurse qualifying examination. In recent years, nurse-education is transferred from the vocational school to the university. Nurse education in the university takes 4-years. Graduation of the university nurse education course gives the eligibility requirements for the national nurse qualifying examination, not only for the nurse, but also for the public health nurse. Eligibility requirements for the national nurse qualifying examination for the midwife are given by finishing the university nurse education course with additional education courses for midwives. A nurse profession association issues the certificates of specialties of nursing in some areas; emergency nursing, cancer chemotherapy nursing, and so on. These may be seen as the same as clinical nurse specialists in other countries.
Fourthly, freedom of choice to utilize any medical institution is guaranteed by laws for all enrollees in the public health insurances. By this, patients by their decision can select a clinic or an outpatient department of hospitals. The free access is assured but it might cause inefficiency in the functioning of clinics and hospitals differentiated. Hospitals with high clinical functioning charge patients for extra fees in addition to the price based on the tariffs for medical care services. This charge is legally permitted. The amount of the surcharge varies from hospital to hospital.
Fifth, the tariffs for medical care services are determined in the Central Social Insurance Medical Council. The Council consists of the representatives of clinical physicians and hospitals, of insurers in public health insurances, and of public interest. Once in two years, the Council determines and updates the tariffs for medical care services as publicly regulated prices. The updates were made by evidences using the results of the Survey for the Financial Situation of the Clinics and Hospitals, and the results of the Survey for the Medical Care Utilization. The update is also the result of the political negotiation, and it is a political inducement tool. When the committee recognizes that there is need for expanding the utilization of some services, but that the low profitability inhibits the provision of the service, then the committee determines to increase its price to induce more medical institutions to provide it. The Ministry of Health, Labor and Welfare decides coverage and tariffs of the medical services, based on suggestion from the council.
Lastly, the medical institution must be non-profit. The notion “non-profit” means that financial surplus from running the medical institution cannot be shared to capital subscriber and/or investor. Financial surplus, if any, must be used for investment to the medical equipment, facilities, etc. or reserved as internal reserves. Exceptionally, private companies own the medical institutions, in order to promote employees’ health. In these cases, the management of those medical institutions must obey a non-profit principle.
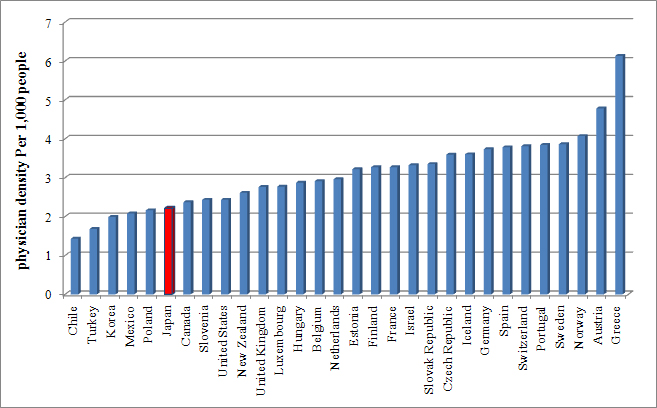
Aging implies that the number of elderly is increasing, who will need not only care for chronic diseases, but also acute care. Since the 1970s, at least one university with a department of medicine was established in each prefecture. It is thought in those days that this policy would satisfy the future need for physician services. However, the increase in medical doctors may not have caught up to the growing need due to rapid aging. As we have seen in section 4.3.2, the total number of medical doctors working in medical institutions is 2.4 persons/1,000 people. This figure is relatively smaller than the ones in OECD countries (Figure 4.2).
This problem is serious in the Tohoku area, which was hit by the Great East Japan Earthquake in 2011. Even before the earthquake, there were relatively few physicians in the Tohoku area. The earthquake hit not only people, but medical personnel and medical institutions as well, so that the number of physicians was decreased after the earthquake. Now it is under the discussion whether a new medical school should be established in the Tohoku area or not.
Elderly people need medical care services and long term care services to support the independent living of the elderly. It is natural to think that both services are supplied to users with good coordination. In this point of view, the establishment of an integrated community care system is needed. To succeed in the establishment of it, communication should be promoted between the personnel in the long term care sector, and the ones in the medical care sector when their services are provided. Section 5.3.2 further explains other points on this.